非小细胞肺癌中的PTEN突变及其与EGFR、ERBB2、KRAS和TP53突变的关系1 z; J8 v6 C+ D1 j( d6 I
PTEN mutations and relationship to EGFR, ERBB2, KRAS, and TP53 mutations in non-small cell lung cancers 4 U2 L7 S# T& u. b$ G+ L
作者:Jin G, Kim MJ, Jeon H-S, Choi JE, Kim DS, Lee EB, # G' j, ~/ `( ]! Y& z
期刊: 《LUNG CANCER》2010年9月3期69卷 ) I- X1 Z& i+ A- W3 o0 y7 ]/ t
" y& U& t+ I- v; T* }* z& y
Somatic mutations of phosphatase and tensin homolog deleted on chromosome ten (PTEN) in non-small cell lung cancers (NSCLCs) have been investigated in but a small number of cases. In addition, the relationship between PTEN mutations and epidermal growth factor receptor (EGFR), KRAS, and TP53 mutations has not been investigated. Therefore, we investigated the frequency of PTEN mutations in 176 surgically resected NSCLCs and analyzed the relationship between PTEN mutations and EGFR, ERBB2, KRAS, and TP53 mutations. Mutations of PTEN (exons 1-9), EGFR (exons 18-21), ERBB2 (exons 19 and 20), KRAS (exon 1), and TP53 (exons 2-11) were determined by polymerase chain reaction and direct sequencing. PTEN mutations were present in 8 (4.5%) of the 176 tumors. PTEN mutations were only found in ever-smokers and were significantly more frequent in squamous cell carcinoma than in adenocarcinoma (10.2% vs 1.7%, P= 0.02). Mutations of EGFR, ERBB2, KRAS, and TP53 genes were found in 36 (20.5%), 2 (1.1%), 11 (6.3%), and 66 (37.5%) cases, respectively. Of the 8 tumors with PTEN mutations, 1 case concurrently had an EGFR mutation and 4 cases had TP53 mutations. However, PTEN mutations were not found in the tumors with KRAS mutation. Our findings indicate that PTEN mutations are relatively common in NSCLC, and thus analysis of PTEN mutations may facilitate a comprehensive understanding of the genetic alterations related to the EGFR signaling pathway.
) _, ~5 S( J6 R; T, e9 R |
 非小细胞肺腺癌四期骨转脑转肝转
非小细胞肺腺癌四期骨转脑转肝转,基因突变KRAS PG-12D,四线治疗安罗替尼耐药,目前
非小细胞肺腺癌四期骨转脑转肝转
非小细胞肺腺癌四期骨转脑转肝转,基因突变KRAS PG-12D,四线治疗安罗替尼耐药,目前
 肿瘤患者化疗期间如何补充营养?(1
化疗药物在杀伤肿瘤细胞的同时难免会伤害一些正常细胞,导致相应的副作用。实际上,并
肿瘤患者化疗期间如何补充营养?(1
化疗药物在杀伤肿瘤细胞的同时难免会伤害一些正常细胞,导致相应的副作用。实际上,并
 ret错义突变可以用普拉替尼吗?
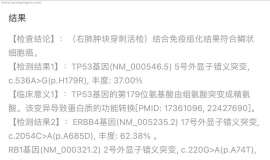
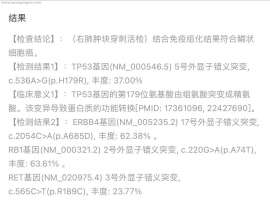
父亲肺鳞癌,无法手术。医院的基因检测报告上提示:肺鳞癌RET基因(NM_020975.4) 3号外
ret错义突变可以用普拉替尼吗?
父亲肺鳞癌,无法手术。医院的基因检测报告上提示:肺鳞癌RET基因(NM_020975.4) 3号外
 求助单免疫纳武利由治疗7个月出现异
病友们大家好大半年没露面了,左肺全切后,免疫治疗马上满一年了,十月份CT显示有17mm
求助单免疫纳武利由治疗7个月出现异
病友们大家好大半年没露面了,左肺全切后,免疫治疗马上满一年了,十月份CT显示有17mm
 请教下 3a 术后 检查
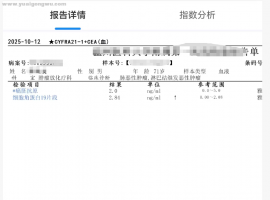
请教下 3a 术后 检查快两年了, 验血 不是每次都是 肿标 5项吗,我的复查 好像 有时
请教下 3a 术后 检查
请教下 3a 术后 检查快两年了, 验血 不是每次都是 肿标 5项吗,我的复查 好像 有时






 显身卡
显身卡 , C5 h8 S( d5 v
, C5 h8 S( d5 v