另一篇 专门讲 怎样战胜特罗凯抗药性的文章。 不知中国能否找到 泛抑制剂HKI-272 和 爱必妥 (后者应当好找)。
+ X) A h$ G6 ?
) F5 d- H! T* ` ADDRESSING TARCEVA RESISTANCE
6 n- R1 M; z5 I8 r% h, ?8 i$ CI. Overview and Background" w6 j1 W/ u% k: I
! z1 ^4 q% _% }: D! [A. EGFR and lung cancer" z# {2 \7 \0 g; D# V
1 W1 b; B5 k8 J% W( Q% g& g' v4 AThe human body has a complex system of signaling between cells with gene duplication a normal part of this process. Duplication is necessary for growth, repair of damaged cells and other functions, and genes signal other cells to initiate replication. Malfunctions in signaling are a critical part of cancer and the tyrosine kinases have been an important target:$ ]. o# U1 Y9 r5 |$ h
9 E& x+ Y" {* I* ^ \# P3 @
Uncontrolled proliferation of tumor cells is a hallmark of cancer. In many types of cancer, mutations in genes that activate cellular signal transduction pathways contribute to enhanced proliferation and survival of cancer cells. One well-characterized example is mutation in tyrosine kinases, enzymes that regulate the growth and survival of cells. Tyrosine kinase activity is tightly regulated in normal cells, but is dysregulated due to mutation in some cancers, including lung cancer, resulting in enhanced proliferation and survival of cancer cells. The tyrosine kinases are attractive candidates for molecularly targeted therapy in cancer, because cancers become dependent on growth signals from the mutant tyrosine kinases. Tyrosine kinases require ATP for their enzymic activity, and thus small molecules that mimic ATP can bind to mutant kinases and inactivate them inveas growth factors prompt excessive carcinogenic cell duplication. Clark (6),7 ~7 B! U$ q0 l% U9 p) V
3 [7 _; h& S9 w8 ]: T
A subgroup of lung cancer patients has a mutation in the epidermal growth factor receptor (EGFR) which is associated with various forms of cancer, particularly lung. Vikis (2). "Recent work has identified a series of somatic mutations in exons 18 to 21 of epidermal growth factor (EGF) receptor (EGFR) that render lung tumors responsive to the gefitinib and erlotinib therapeutics." Vikis (2). These people are EGFR positive, as measured by a sensitive EGFR mutation test. See Harvard EGFR test.
+ M8 y- @ r y3 y- d2 g) m: `1 a% ]0 B' n
The response rate to Tarceva for EGFR positive patients is approximately 60%, with response rates further varying upon the particular exon(s) on which the mutation is located. EGFR positive patients are principally but not exclusively non-smokers with adenocarcinoma. Some light former smokers and a few squamous cell patients are EGFR positive. EGFR positive patients appear to have tumors driven by aberrant EGFR signaling. with oncogene addiction, a plausible theory.9 ^/ B# z, ^+ D6 l; s: {
2 `2 H0 q1 p: l, D$ aThe EGFR is a part of the Erb family of receptors. Cross-signaling among the other receptors including Erb2 occurs, though the precise role of the other receptors in lung cancer is unclear./ @9 k! ^4 E2 {1 ^) Z+ X- ?
6 a) M- ~' K5 tWhile the initial response rate to Tarceva is impressive with partial and even complete responses, (total elimination of any visible tumor on Ct to the drug) many patients develop resistance and Tarceva becomes effective. Why do patients develop resistance and what can we do about it are the questions.
) V+ Z; _" O8 M6 }6 L* s
# a# T ~5 x4 m2 i, r5 t7 F4 h( G1 ]/ Z- W
II. The Development of the T790M Mutation
! s9 {/ f3 p% Q* S8 t) n2 v" U/ m' `! ~+ a& ~( I
A. T790 Mutation: t: u2 h. g) n' k! A0 i4 x
, D! t: K+ e9 o2 m$ m7 |However, many patients who initially respond to Tarceva find the drug is no longer effective. One cause appears is the development of a Tarceva-resistant EGFR mutation at T790M. "The use of tyrosine kinase inhibitors (TKI) has yielded great success in treatment of lung adenocarcinomas. However, patients who develop resistance to TKI treatment often acquire a somatic resistance mutation (T790M) located in the catalytic cleft of the epidermal growth factor receptor (EGFR) enzyme." Vikis (2). "In patients that progress after drug treatment, it has been observed that a secondary "resistance" mutation is often acquired in exon 20 (4–6). This mutation, T790M, arises somatically in 50% of these cases." Vikis (2). The change involves threonine-to-methionine substitution at amino acid position 790 (T790M) of the epidermal growth factor receptor (EGFR) gene." Inukai (3). "About half of the acquired resistance to EGFR-TKIs that almost always occurs during the course of treatment is caused by a secondary mutation at codon 790 (T790M)." Fukui (8).9 {1 n& q4 p: {; b4 W
6 ]- Q) v! r- }) a$ R" m
B. Rationale for Testing and Characteristics of the T790 Mutation. P" r9 T" c Y% t1 Z" k, {
The T790m mutation plays an important but not exclusive role in generating resistance to Tarceva. It makes sense to determine its impact upon a particularly patient. See gxsgenetyping.com<http://gxsgenetyping.com/> outlining its T790 test. It may make sense to test patients taking Tarceva yearly for the mutation, or at least when it appears Tarceva is no longer effective.
3 r S0 T" o5 M, v3 r S* \9 i2 \4 F+ _
1 `- F' v/ r9 k3 N$ g& h, r
"The T790M test uses a combination of Scorpions® and ARMS® (allele specific PCR) technology. This approach allows the development of very sensitive tests that can detect mutations in a background of normal cells. The real-time PCR based test enables rapid identification and quantification of the mutations. Mutations can be detected at a ratio of 1:100 mutant: normal DNA and this allows the kit to detect genetic variation that could not be detected using DNA sequencing methods." dxsgenotyping.com<http://dxsgenotyping.com/>
. {% M2 ]1 n/ c G0 B$ g" Y; X8 o, j
% m3 S0 w+ }1 ?; I# ]
III. Pan-Inhibitors+ ?7 s6 G0 g! K) q& u) [1 Y
8 ~) p; z: {0 m
A. Overall Approach# F; {$ O$ ^9 ?- f: x1 c n9 _
3 H6 a, z, E, C3 L0 b/ {2 v( a
Pan-inhibitors have shown some success in cell studies in suprresing T790 resistance. Sharma explains:' q) M4 p& Z" N t! x4 Z: t! i7 O
9 Y* k' x2 ~# E6 t) \, b# o# I9 C# M' ~5 V
- T' i. f8 k/ Z"one of the main challenges in the treatment of NSCLC is to design inhibitors that can overcome the steric interference to drug binding conferred by the T790M mutation. Irreversible inhibitors seem to show some promise in this regard. In most cases, irreversible inhibitors form a covalent bond with crucial cysteine residues — Cys797 within EGFR or Cys805 within ERBB2 — in the active site of the respective enzymes. Given the fact that only EGFR and ERBB2 (as opposed to ERBB4) have cysteines at these corresponding positions, irreversible ErbB inhibitors show very high specificity for EGFR and ERBB2. Previous studies from our laboratory have shown that the irreversible dual EGFR and ERBB2 inhibitors, HKI-272 (Ref. 136) and HKI-357 (Ref. 37), as well as the irreversible EGFR inhibitor EKB-569 (Ref. 137) were all able to overcome gefitinib resistance owing to T790M in cis with an L858R mutation in EGFR. Sharma (5)( c; J/ P( l9 r' e, Y& P% \
|
 各位朋友,我爸爸没有靶向药,pdl只
各位朋友,我爸爸没有靶向药,pdl只有百分之5,这个医治率高不高,我爸爸是肺腺癌,寡
各位朋友,我爸爸没有靶向药,pdl只
各位朋友,我爸爸没有靶向药,pdl只有百分之5,这个医治率高不高,我爸爸是肺腺癌,寡
 25次放疗后,她亲手写下6点放疗战胜
作者:深色系
放疗是通过放射线的电离辐射作用杀灭肿瘤细胞的一种局部治疗方法,它几
25次放疗后,她亲手写下6点放疗战胜
作者:深色系
放疗是通过放射线的电离辐射作用杀灭肿瘤细胞的一种局部治疗方法,它几
 肺动脉阻塞,胸闷气短,下一步如何处
请教各位有经验的友友们,目前这种情况如何处理?现在气短的厉害,已无法正常行走,走
肺动脉阻塞,胸闷气短,下一步如何处
请教各位有经验的友友们,目前这种情况如何处理?现在气短的厉害,已无法正常行走,走
 一位肿瘤科护士的硬核抗癌路:4次基
讲述者:阿雷一点都不累整理者:Tony
2023年12月28日那一天,我34岁的妹妹被确诊为Ⅳ
一位肿瘤科护士的硬核抗癌路:4次基
讲述者:阿雷一点都不累整理者:Tony
2023年12月28日那一天,我34岁的妹妹被确诊为Ⅳ
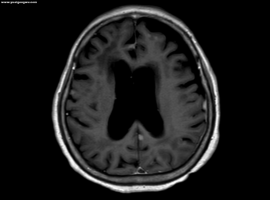 L861Q多发脑转和脑膜转使用佐利替尼
患者是我妈妈,今年71岁,治疗经过如下:
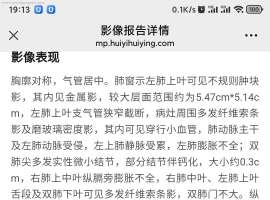
2023-6-7 确诊右肺上叶肺腺癌伴多发淋巴结、
L861Q多发脑转和脑膜转使用佐利替尼
患者是我妈妈,今年71岁,治疗经过如下:
2023-6-7 确诊右肺上叶肺腺癌伴多发淋巴结、






 显身卡
显身卡

 高高兴兴是一天,愁眉苦脸还是一天,就看如何选择。生命会随着时间的流失而慢慢远去的,珍惜现在的每一天,过好每一天是最重要的,别给自己吃后悔药。
高高兴兴是一天,愁眉苦脸还是一天,就看如何选择。生命会随着时间的流失而慢慢远去的,珍惜现在的每一天,过好每一天是最重要的,别给自己吃后悔药。


