| |
|
个人公众号:treeofhope
|
|
点评
建议空窗,定期检查,出现情况时再上易瑞沙吧,鸦胆子油没啥用。
| |
| |
| |
|
个人公众号:treeofhope
|
|
| |
|
个人公众号:treeofhope
|
|
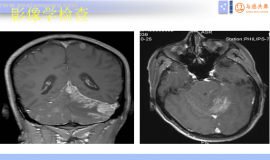
 脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结
脑膜转移 中位治疗生存期 3-6月
脑膜转移的临床表现
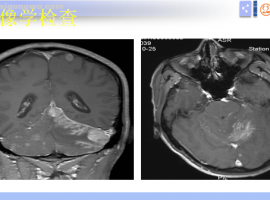
脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结
脑膜转移 中位治疗生存期 3-6月
脑膜转移的临床表现
 肺腺癌egfr19+骨转移,这样治疗可以
病情与治疗过程概述
患者年龄58岁,男性,已戒烟30年
1. 确诊情况(2025.05.26):患
肺腺癌egfr19+骨转移,这样治疗可以
病情与治疗过程概述
患者年龄58岁,男性,已戒烟30年
1. 确诊情况(2025.05.26):患
 肿瘤患者出现水肿,11种缓解方法请收
作者:闵水肿是中晚期肺癌患者比较常见的一种副作用,它不仅影响美观,还给不少病友的
肿瘤患者出现水肿,11种缓解方法请收
作者:闵水肿是中晚期肺癌患者比较常见的一种副作用,它不仅影响美观,还给不少病友的
 卡度联合安罗,谁让肿瘤缩小了
肺低分化腺,伴肉瘤样。卡度尼利单抗联合安罗替尼。两个疗程复查显示肿瘤缩小,胸膜增
卡度联合安罗,谁让肿瘤缩小了
肺低分化腺,伴肉瘤样。卡度尼利单抗联合安罗替尼。两个疗程复查显示肿瘤缩小,胸膜增
 父亲确诊“癌王”生命危在旦夕,医护
讲述者:吉吉整理者:pear
一年前,父亲被确诊为胰腺癌伴肝转移,那一刻,我的人生仿
父亲确诊“癌王”生命危在旦夕,医护
讲述者:吉吉整理者:pear
一年前,父亲被确诊为胰腺癌伴肝转移,那一刻,我的人生仿





 显身卡
显身卡