abstract:
P3.02c-048 - A Phase I/II Trial Evaluating the Combination of Stereotactic Body Radiotherapy and Pembrolizumab in Metastatic NSCLC
Background:
Immune checkpoint inhibitors are taking on a growing role in the treatment of patients with metastatic NSCLC. Pre-clinical evidence suggests that radiotherapy may increase the frequency, or enhance the strength of the host anti-cancer immune response. We report the preliminary results of an ongoing phase I/II trial combining stereotactic body radiotherapy (SBRT) and the anti-PD-1 antibody pembrolizumab in patients with metastatic NSCLC.
Methods:
Eligible patients are those with metastatic NSCLC who have received no prior immune-directed therapy, and have at least 2 sites of measurable disease as per RECIST 1.1. PD-L1 expression is not required for study entry. All patients are treated with pembrolizumab at 200 mg every 3 weeks until development of progressive disease by immune-related RECIST criteria (irPD). After irPD, patients receive SBRT to a single site of disease and continue pembrolizumab. The primary endpoint is safety and tolerability. Secondary endpoints include the pre- and post-SBRT overall response rate.
Results:
27 patients with advanced NSCLC have enrolled and started trial therapy. The overall response rate (irPR and irCR) to the initial course of pembrolizumab is 35%. To date, 13 patients have had irPD: 5 were not eligible for SBRT and stopped study treatment (2 developed new brain metastases, 3 had decline in PS), and 8 patients received SBRT to a single site of disease (6 thoracic, 1 adrenal, 1 vertebral) and continued pembrolizumab. 5 of these patients are evaluable for post-SBRT response: 1 patient had confirmed irPD, 4 have irSD and continue pembrolizumab post-SBRT at a median duration of 3 months (range 1 to 5 months). 2 of the 4 patients with irSD have had > 20% decrease in the sum of diameters of their unirradiated targets, since SBRT. Regarding adverse events, in the pre-SBRT phase 6 of 27 patients (22%) developed grade 3 treatment-related toxicity (2 colitis, hepatitis, pneumonitis, hypothyroidism, conjunctivitis). In the SBRT and post-SBRT phases, there have been no grade 2 or greater treatment-related events.
Conclusion:
The addition of SBRT to pembrolizumab has not resulted in an increase in treatment-related toxicity. Several patients who had serially confirmed irPD to pembrolizumab monotherapy underwent SBRT and now have irSD, with some evidence of tumor regression. Updated results will be presented.
combination of erlotinib and atezolizumab有更稳定的实验效果
Safety, Clinical Activity and Biomarker Results from a Phase Ib Study of Erlotinib plus Atezolizumab in Advanced NSCLC
Background:
Targeted therapy with erlotinib is effective in reducing tumor burden in EGFR-mutant non-small cell lung cancer (NSCLC). However, resistance to therapy develops almost universally. Atezolizumab, an engineered mAb that inhibits binding of PD-L1 to its receptors, PD-1 and B7.1, has demonstrated promising monotherapy activity in NSCLC. Given that atezolizumab may enhance and perpetuate anti-tumor immunity, we hypothesized that combining atezolizumab with erlotinib may improve both clinical response and durability in EGFR-mutant NSCLC.
Methods:
This Phase Ib study consisted of a safety-evaluation stage in patients with NSCLC regardless of EGFR status followed by an expansion stage in TKI-naïve patients with tumors harboring activating EGFR mutations. Patients were enrolled regardless of PD-L1 status. After a 7-day run-in with 150mg erlotinib PO QD alone, patients received 150mg erlotinib PO QD and 1200mg atezolizumab IV q3w. To evaluate immune biology, biopsies were obtained in expansion-stage patients pre-treatment, after erlotinib run-in, at weeks 4-6, and at progression. The primary objective was to evaluate the safety and tolerability of the combination. Secondary objectives included evaluation of the clinical activity per RECIST v1.1. Data cutoff, 11 April 2016.
Results:
Twenty-eight patients (safety stage, n = 8; expansion stage, n = 20) who received ≥ 1 dose of erlotinib or atezolizumab were considered safety evaluable. Median age was 61y (range, 47-84); median survival follow-up was 11.2mo (range, 0.8-24.2). The incidence of either treatment-related G3-4 AEs was 39% and for serious AEs, 50%. The most common atezolizumab-related G3-4 AEs were pyrexia and increased ALT. No pneumonitis was reported. No treatment-related G5 AEs occurred. Five patients discontinued atezolizumab due to treatment-emergent AEs. No DLTs were observed. In the expansion-stage population, ORR was 75% (95% CI, 51-91). Disease control rate (CR + PR + SD ≥ 24 weeks) was 90% (95% CI, 68-99), median PFS was 11.3mo (95% CI, 8.4-NE) and median DOR was 9.7mo (range, 4.2-11.7). Increases in intratumoral CD8+ T cells post-erlotinib run-in were observed in 8/13 evaluable paired biopsies. Higher intratumoral CD8+ T-cell prevalence and immune gene expression signatures at baseline were associated with improved PFS.
Conclusion:
The combination of full dose erlotinib plus atezolizumab demonstrated a manageable safety profile. While response rates and median PFS for combination treatment appear similar to those observed with erlotinib monotherapy, the addition of atezolizumab to erlotinib may lead to more durable clinical responses in some patients. Additional follow-up is required to evaluate the full potential of this combination treatment.
: http://library.iaslc.org/virtual ... ;author=&catego ry=&date=&session_type=&session=&presentation=P3.02c-046&keyword=atezolizumab
肿瘤也会侵吞蛋白质,不给免疫系统和身体,随着肿瘤长大侵吞的蛋白质越来越多?
有人认为趁着肿瘤不大(早期),用免疫疗法消灭散布的无形的肿瘤细胞,消灭不掉的就冷冻消融,肿瘤越大肿瘤杀灭率越高。
一个07年患上肿瘤,依靠免疫治疗生活,存活的人的主页:
http://curingcancerbook.com/how-i-survived-cancer-immunotherapy
SBRT或许可以用于早期的,肿瘤不大于5cm的,不包含淋巴结的情况,认为这也许是可行的有效的选择,对那些EGFR早期阶段并且不是外科手术候选人并有显著伴随疾病的人。
http://library.iaslc.org/virtual ... uthor=&category
用放射治疗和免疫治疗抑制剂联用,会增加患者对免疫治疗的应答率?
实验阶段,但是这种治疗有过极大收益的案例(把人从死亡线那里拉回来的案例)
排序也许是放射治疗和免疫治疗联用成功的关键。
肿瘤也会侵吞蛋白质,不给免疫系统和身体,随着肿瘤长大侵吞的蛋白质越来越多?
有人认为趁着肿瘤不大(早期),用免疫疗法消灭散布的无形的肿瘤细胞,消灭不掉的就冷冻消融,肿瘤越大肿瘤杀灭率越高。
一个07年患上肿瘤,依靠免疫治疗生活,存活的人的主页:
http://curingcancerbook.com/how-i-survived-cancer-immunotherapy
SBRT或许可以用于早期的,肿瘤不大于5cm的,不包含淋巴结的情况,认为这也许是可行的有效的选择,对那些EGFR早期阶段并且不是外科手术候选人并有显著伴随疾病的人。
http://library.iaslc.org/virtual ... uthor=&category
用放射治疗和免疫治疗抑制剂联用,会增加患者对免疫治疗的应答率?
实验阶段,但是这种治疗有过极大收益的案例(把人从死亡线那里拉回来的案例)
排序也许是放射治疗和免疫治疗联用成功的关键。
肿瘤也会侵吞蛋白质,不给免疫系统和身体,随着肿瘤长大侵吞的蛋白质越来越多?
有人认为趁着肿瘤不大(早期),用免疫疗法消灭散布的无形的肿瘤细胞,消灭不掉的就冷冻消融,肿瘤越大肿瘤杀灭率越高。
一个07年患上肿瘤,依靠免疫治疗生活,存活的人的主页:
http://curingcancerbook.com/how-i-survived-cancer-immunotherapy
SBRT或许可以用于早期的,肿瘤不大于5cm的,不包含淋巴结的情况,认为这也许是可行的有效的选择,对那些EGFR早期阶段并且不是外科手术候选人并有显著伴随疾病的人。
http://library.iaslc.org/virtual ... uthor=&category
用放射治疗和免疫治疗抑制剂联用,会增加患者对免疫治疗的应答率?
实验阶段,但是这种治疗有过极大收益的案例(把人从死亡线那里拉回来的案例)
排序也许是放射治疗和免疫治疗联用成功的关键。
当和免疫治疗联合,比如免疫检查点阻断,局部的放射可以有效的使患者正在照射的肿瘤有免疫性,改变肿瘤成为一个个性化的situ vaccine,当成功了,这获得的免疫反应加强注射在被放射的肿瘤和其相邻区域中。(可以与注射了疫苗后获得的对病毒性和细菌性感染的抗拒相比较)。
有认为,在肿瘤的位置,肿瘤细胞被嵌入在一个普遍免疫抑制的环境,这难以破坏。放疗被广泛的用来作为一个抗癌的物理疗法,注重于射线对肿瘤和对微环境的摧毁效果。
免疫治疗和放疗联合的方法对乳癌和非小肺癌有效的比较多。具体网址:
http://www.cancernetwork.com/onc ... herapy-treat-cancer
PD-L1检查的名称:protein expression by immunohistochemistry (IHC)
射波刀之类的local consolidation therapies 一般用于局部和 oligometastatic cancer (在诊断时少于三处lesions或更少)
local consolidation therapies 绝不该做当患者正经历一个系统性的进展时(systemic progression)或者是这个患者lesion的位置不好不能被外科治疗或者放疗()(和上面有关)()()()
scientists inject modified cells into patient with agressive lung cancer:
http://www.nature.com/news/crisp ... -a-person-for-the-f irst-time-1.20988?WT.mc_id=FBK_NatureNews
肿瘤进展的时候会在血液中释放更多DNA可以被检测到?
如果CEA没达到5,也许是个不够敏感的检测指标,关于指标的一个网址,可以找到一部分指标:
https://www.inspire.com/groups/a ... -lung-cancer-surviv ors/discussion/sharing-experience-on-blood-markers/
一个关于nivo的讨论:
https://www.inspire.com/groups/a ... -lung-cancer-surviv ors/discussion/nivoluamb-club-members/
NK cell therapy(NK细胞疗法关于免疫治疗):
http://jitc.biomedcentral.com/articles/10.1186/s40425-016-0172-7
pneumonia(肺炎)有时候不是感染性的并且可以是药物导致的、或由免疫系统引起的、或还有其他理由(copd等),找到导致肺炎的最初原因很重要。方法有细菌的痰培养、gram stain test、病毒培养(viral culture)、真菌试验(fungal test)、(blood culture )、胸腔积液分析(pleural fluid analysis)等。
有关itraconazole 的网址:
http://ecancer.org/journal/9/ful ... in-oncology-redo-it raconazole-as-an-anti-cancer-agent.php
一些去年EMSO会议的摘要有关osimertinib and hedgehog inhibition (itraconazole is a hedgehog inhibitor)
在inspire上讨论的不同的thread
https://www.inspire.com/groups/a ... -lung-cancer-surviv ors/discussion/immunotherapy-with-dendritic-cells-and-newcastle-disease-vir us/reply/6015865/?reply_sort=desc
一个阶段二的培美曲塞和itraconazole作为转移性的NSCLC二线治疗
https://www.ncbi.nlm.nih.gov/pubmed/23546045
一些作用在肺上的药物也许会对胸膜有伤害
治脚趾手指的副作用的药物:叫 Nemycin and Polymyxin Sulfates and Hydrocortisone Otic Solution, USP。
把手脚浸泡在盐水里防减少不适?也许会需要抗生素,取决于情况的严重程度。看足病医生
在指甲刚刚红痒的时候
Itraconazole也许可以停止NSCLC的增长,通过阻塞新生血管对于肿瘤生长必要的,并阻塞一些细胞生长需要的酶:
https://www.cancer.gov/about-can ... rials/search/view?c drid=769055&version=HealthProfessional&protocolsearchid=15349411
关于伊曲康唑的描述:In general, itraconazole is a synthetic triazole agent with antimycotic properties(抗真菌特性)。Formulated for both topical and systemic use, itraconazole preferentially inhibits fugal cytochrome P450 enzymes, resulting in a decrease in fungal ergosterol synthesis. Because of its low toxicity profile, this agent can be used for long-term maintenance treatment of chronic fungal infections(因为低毒性,可以被用于长期慢性真菌感染).
然而伊曲康唑散布在polymer matrix中,是一个proprietary oral formulation,有抗真菌的和潜在的抑制血管生成的活动,口服后抑制enzyme cytochrome P450 lanosterol 14 alpha-demethylase导致真菌角麦固醇合成的减少,尽管伊曲康唑抑制血管生成彻底的机制至今还没有完全的说明,这个药剂显示出抑制hs信号通道,胆固醇合成和哺乳类mtor发信号的靶向在内皮细胞里。这个药剂也许也阻碍,
如果抑制那个hs信号通路,
如果KRAS是导致9291耐药的原因,EGFR MEK联用也许是可行的策略。
之前有用特罗凯后耐药,用Cetuximab和afatinib联用有很好的效果,除了每天30mg的afatinib,Cetuximab 250mg/m2 每两周。250mg的剂量需要乘以每个人的BSA来获得每次注射的总体剂量。接受过两次400mg的剂量每年(或接种过两年疫苗?)或接受过两年的400mg的剂量每两周。
Preliminary results from gene analysis revealed appearance of SMO gene mutation (V404M) in one tumor resistant to afatinib and in the tumor resistant to osimertinib, with a concomitant activation of the Hedgehog pathway.
NCI实验搜索的网址
https://www.cancer.gov/about-can ... rials/search/result s? protocolsearchid=8640293
Sonidegib is an orally bioavailable small-molecule smoothened (Smo) antagonist with potential antineoplastic activity这个药有潜在的抗肿瘤效果。原理:(Sonidegib selectively binds to the hedgehog (Hh)-ligand cell surface receptor Smo, which may result in the suppression of the Hh signaling pathway and, so, the inhibition of tumor cells in which this pathway is abnormally activated. The Hh signaling pathway plays an important role in cellular growth, differentiation and repair. Inappropriate activation of Hh pathway signaling and uncontrolled cellular proliferation, as is observed in a variety of cancers, may be associated with mutations in the Hh-ligand cell surface receptor Smo.)
在小鼠模型中,西妥昔单抗(或selumetinib)趋向延长反应对osimertinib。
ctDNA是一个有力的代替来检测NSCLC患者的EGFR突变
测试9291与阿法和选择性SMO抑制剂联用的效果
I noticed, on the pages you mention, in particular the research (several abstracts) on the hedgehog pathway done by this research group in Naples. Here is one of the abstracts (abstract 8P):
"Efficacy of osimertinib in combination with Hedgehog pathway inhibitors in reverting T790M-mediated resistence
G. Esposito, C.M. Della Corte, F. Papaccio, G. Viscardi, M. Fasano, T. Troiani,
E. Martinelli, F. Ciardiello, F. Morgillo
Medicina Clinica Sperimentale Magrassi Lanzara, AOU Seconda Università degli
Studi di Napoli (AOU-SUN), Naples, Italy
Background: We have previously found that Hedgehog pathway plays an important
role in mediating resistance to first, second and third generation EGFR tyrosine kinase
inhibitors (EGFR-TKIs), suggesting new potential strategies of combination of novel
generation EGFR-TKIs with Hedgehog inhibitors to prevent the occurrence of
resistance in T790M + tumors.
Methods: H1975-AFAR and –OSIR NSCLC cell lines, harboring both the EGFR
activating (L858R) and the resistant (T790M) mutations at baseline, were developed in
vivo by continuos treatment with afatinib and osimertinib respectively. Both cell lines
presented also the SMO V404M mutation after acquisition of resistance. These cell
lines were used to test the efficacy of osimertinib or afatinib in combination with the
selective SMO inhibitor, LDE225.
Results: Treatment with each EGFR-TKIs in combination with LDE225 resulted in a
significant inhibition of cell proliferation and a strong induction of apoptosis as compared
to single agent treatment. Additionally, combined treatment significantly decreased the
invasive and migratory abilities of resistant cells. The combination of osimertinib and
LDE225 appeared to be the most effective in reverting resistance to EGFR-TKIs. Combined
treatment caused regression of tumor growth in vivo in nude mice.
Conclusions: Our study further support the role of Hedgehog pathway activation as an
important mediator of resistance to EGFR targeting drugs, also in the T790M scenario.
In addition, it demonstrates that addition of a hedgehog inhibitor to an EGFR-TKI in
tumors, which had developed resistance to third generation inhibitors, provides
meaningful responses."
认为这个hs信号通道和调节TKI naiyao有关。(还是有必要打击?效果不一定)
https://www.ncbi.nlm.nih.gov/pubmed/20385363
一个实验“OS、OR或PFS之间的关系在进展的被用以抑制PD-1\PD-L1抗体治疗的患者中。”这个实验认为用PD1\PDL1的患者在8,6或24周的scan中起效,效果会比较好。
PIK3C占据一个上游的位置横跨两个独立的通道:ACT/mTOR和MAPK/ERK.
有做化疗敏感实验(RGCC chemo-sensitivity tests),认为依维莫司和西罗莫司脂化物(temsirolimus)都不会起到效果。通过实验认为MEK抑制剂被假设会其效果。
PIK3C激活RAS/RAF/MEK/ERK信号通路(也被叫做MAPK/ERK)
相关图片在这个22页
https://www.inspire.com/groups/a ... amp;reply_sort=desc
类固醇(steroids)用来调低免疫。用伊匹单抗引起的副作用,使用类固醇挺有效。
类固醇会影响TKI(靶向)?
有两个PD-L1不表达的NSCLC用了keytruda和一种新药联用后中位无进展生存期9.3月,有达14个月(很长)的随访期。值得注意就是PD-L1不表达的NSCLC用keytruda好像一般效果不好,但这里效果很相反。
具体网址:
http://www.prnewswire.com/news-r ... ence-300334063.html
关于cimavax和vaxira 目前暂时没看到有明显效果的回复。
关于化疗的一些看法:
https://academic.oup.com/annonc/ ... ssential-element-of
化疗是系统的治疗。很多化疗药物会有损耗的效果对于免疫系统。
lesion小于2cm用射波刀,伤害较小认知性损伤也较小。(?)
LIT,一种和放射有关的疗法。
一些效果:https://www.odt.co.nz/news/duned ... apy-treatment-hopes
关于LIT的详细资料包括应用等:
http://www.ajnr.org/content/early/2015/06/25/ajnr.A4362.full.pdf
NDV和dendritic cells联用是一个方法。
9291不像化疗按周期来,不该在准备换药时等到9291的周期结束。
脑转治疗后产生的放射性坏死有可能会进展,长时间后进展的也有,但是这种坏死难以被PET/CT发现,要用活检和微观检测(microscopic examination)。也有有关MRI的检测建议。
检测报告上的皮质只是为了弄清lesion生长在头部(brain),而不是头(head)的其他部分上。
Vasogenic edema血管性水肿,可能是放射性坏死(necrosis)或necrosis再发展造成的
在放射治疗后,复发的肿瘤单独的和放射性坏死和肿瘤结合起来有两倍的发生的可能性比起纯粹的放射性坏死。在传统的MR图片中,发现有很高程度的重叠在放射性坏死和复发的肿瘤之间。技术发展帮助更好的辨别放射性坏死和复发肿瘤之间的不同,但个体诊断依旧因而复杂。
具体网址:http://pubs.rsna.org/doi/full/10.1148/rg.325125002#_i7
使用te之类的,向医院寻求治疗会避免造成的问题(副作用)更加严重,医生会用皮质类固醇(corticosteroid)或荷尔蒙(hormone)代替更换药物,会停止或延迟te使用。
te药要求使用过含铂化疗,并且突变基因还存在。
脑转推荐伽马刀可被用很多次,尤其是只有一小部分lesion被治疗过。
培美和nitrosoureas已知可以跨越BBB。当卡铂与培美联用,这可以帮助培美跨越BBB。blood brain barrier
LIT治疗显然是一个最低侵略性的程序(要打开头盖骨5mm,插入探针burn lesion)。LIT通常被认为是最好的选择治疗recurrent brain met。
Whole Tumor Antigen Vaccines的网址:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4494356/
理论性很强。
疲劳有可能是副作用或是胸水没抽干净。
“TKI-vacation”也许会突然加重胸水?(不一定)
关于TKI的副作用管理:
皮肤(所有TKI)
TKI皮疹用口头或局部治疗(Minocycline二甲胺四环素,Doxycycline多西环素都是100mg,克林霉素—局部的),或一个局部的类固醇cream(Clobetasol Propionate 0.05%等)。TKI皮疹不是痤疮,用痤疮产品会加重情况?
一些皮疹在身体上,并在皮肤的皱纹和折痕里可能会变成真菌感染,他们治疗的越快越好。
athlete’s foot 和 jock itch
Use OTC products for athlete’s foot and jock itch. Expose to air 2 – 3 time a day. Use fungal powder to avoid future outbreaks.
干皮肤(大部分TKI)
O’Keefe’s Working Hands, Udderly Smooth , CeraVe, Eucerin to name a few. Argan or coconut oil are effective, too.(也许需要一些实验才能找到有效用比较高的。)
Kenalog (script)对于非常痒的rash。问医生其他的steroid creams and lotions。可以看皮肤科医生,只要看对TKI熟悉的医生就可以。
头部
掉头发、头发会改变质地等,长的很慢。
面部毛发
轻微的可以用OTC
头皮皮疹或结痂
Zinc Shampoo DHS 香波,(script and available OTC), Ciclopirox 1% Shampoo (script), Capex Shampoo (script) Olux Foam Shampoo (script). Note that sun, heat and perspiration can make the scalp rash worse.
香波护发素的使用
避免有酒精含在里面?
眼部
Tarceva users should beware of wiry, rogue eyelashes that bend(弯曲) and wind up hitting your eyeball and infected or ingrown lashes. Contact your ophthalmologist.(眼科的医生)
刺激/干燥
温暖的敷布对于滑腻的、硬的早晨的眼睛。
在刺激持续几天之前去找眼科医生,TKI有角膜炎的副作用。
白内障更为普遍,在TKI使用者中,一段时间去看一次眼科医生。
鼻子和嗓子
气短,告诉医生,TKI有小风险的间质性肺病。
流鼻水
Claritin Allergy Relief or Flonase for drippy nose.
cotton buds smearing up the nose(乳头霜和棉花芽涂抹鼻子)
-------------------------------------------------------------------------------------------
bleeding nose
mothers nipple cream on cotton buds smearing up the nose
鼻孔溃疡(sore)
Neosporin, Ayr (OTC gel) or Futacason (script) on a Q-tip inside nostrils.
嘴部(溃疡或干燥)
Magic Swizzle Sticks from Pharmacy. Mix equal parts of Peroxide and Water and gargle daily. Magic Mouthwash, Stomatitites Cocktail, Vanderbilt Formula (scripts).
Diflucan (script) for Oral Thrush (which is a whitish fungal infection coating on your tongue). Do call the onc for this one!
Biotene toothpaste and mouth rinse (both OTC) for dry mouth. Toothpaste is very gentle for mouths with sores.
Tarceva users in particular find that the taste of certain foods (spicy or acidic) will change. This should decrease over time.
小苏打可以当柔软的牙刷,小苏打和水混合(口腔清洗)
胃酸
看医生。Tarceva in particular works with the acid in your stomach. While relief is important, it shouldn’t interfere with the Tarceva
便秘
番泻叶天然泻药,Miralax, Colace and Fiber Gummies.
腹泻
易蒙停和益菌(Probiotics),止泻宁,加一些通便的可以有帮助(美达施,psyllium husk fiber等。)??Use the BRATT (bananas, rice, applesauce, toast and tea) to help calm things down.
UPET STOMACH – ginger tea, peppermint tea, coke syrup (pharmacy OTC), Carafate (script).胃不舒服胃痛?
胃口
当有胃口时吃含卡洛里尽量多的食物。
腿痛性痉挛
医生应当做一个CBC检查身体里元素含量水平。
手指和脚趾
保持脚干净干燥、保持指甲是修正过的、穿舒适宽松的鞋。
如果手指或脚趾的角质层看起来发炎或感染了,找足病医生,有可能是甲沟炎并且感染也许会变得严重。向内生长的脚趾甲也是常见的副作用,告诉足病医生?
Vaseline, Amonium Lactate 12% for cracked heels and feet. Epsom Salt soaks are helpful, too.
清理的时候用橡胶手套,一些需要注意的
Newskin, Nexcare or other waterproof bandages for split fingers and heels.
Desitin (yep, diaper rash cream) applied thinly to fingertips and a bit thicker other places.
Super glue (medical grade) for splits, too.
Moisturize、睡觉的时候带上棉手套、袜子。
如果感受到副作用加重或其他的副作用,找医生,在用别的药物移除这些副作用之前也要找医生,让你知道是什么副作用,并立刻做出应对。
一些有用的链接
The Tarceva Patient Information link: http://www.tarceva.com/patient/
The Tagrisso Patient Information link: https://www.tagrisso.com/
The Iressa Patient Information link (U.S.): https://www.iressa-usa.com/
The Gilotrif Patient Information link: http://www.gilotrif.com/
Source for checking drug interactions (click on interaction tab):
http://www.drugs.com/cdi/tarceva.html
一个解释TKI如何运作的链接:
http://www.cancerresearchuk.org/ ... general/treatment/b iological/types/cancer-growth-blockers#tki
关于特罗凯:
http://www.inspire.com/groups/lu ... ussion/tareceva-sid e-effect-busters-4
https://www.inspire.com/groups/a ... -lung-cancer-surviv ors/discussion/tarceva-side-effect-busters-5/
Eliminate or cut down on potassium rich foods like bananas, spinach, tomatoes, chocolate, fresh salmon, etc.
Dexamethsone 0.5mg/5ml mouthwash, it is a preventative unlike magic mouthwash that is used after sores have developed.
关于吃药饭前饭后
对于脚的部分
Epson Salts A & D ointment (found in baby department) mixed with vitamin D oil to feet
polysporin, tea tree oil, epsom salts, soaking
冰袋管用吗?
soaked nail beds in water and vinegar twice a day...used exelderm and Mupirocin有很不错的帮助
used liquid bandages to ease the pain in fingers. Next started with a fungal infection in big toes. Now have Paronychia. You need a good antibiotic and need to soak your hands or effected feet in hot water ( Salted) to draw out inflammation. Depending on how infected it will need to be drained.
Fluoxycillian
甲沟炎
Bactrim效果很好过
关于指尖
一天浸透3-4次每次十分钟的指尖在有Epsom salts and a bit of coconut oil thrown in. coconut oil是一个自然的方式来治疗手指感染。(有一天内状况好了不少的)
put neosporin on the splits, slip on the cots, apply argon oil to the rest of my uncovered fingers & my hands
关于流鼻水
I have a constantly runny nose and was getting sores.minstarted using tissues infused with lotion (puffs and Kleenex both make them) and the sores no longer form.
头皮
Scalpicin药物的名称
穿棉的舒适的衣服
对于nimples需要保湿
皮疹
Gold Bond powder对皮疹很有效?减少发痒?一直保湿也很重要
驱动基因一般只有一个,如果需要选择新药了,仔细检查molecular testing的结果,要做biopsy和基因组面板(genomic panel)这两样。
要用PD-1/PD-L1抑制剂必须经历过化疗。
FDA也推荐了pd1/pd-l1抑制剂给squamous cell carcinoma type lung cancer类型患者。
关于脑转的治疗
显著提高的脑转PFS在EGFR TKI的治疗下:
https://www.inspire.com/groups/a ... -fight-is-still-on/
FDA正在加速批准Keytruda和培美曲塞、卡铂联用作为一线(frontline)治疗对于转移性的、进展性的非鳞NSCLC患者,无视PD-L1的表达。
http://www.curetoday.com/article ... %20story%20%5Cu00BB
FDA批准Portrazza用于鳞癌。
ROS1积极患者可以用crizotinib作为一线用药。
https://www.inspire.com/groups/a ... arch-lcam-and-hope/
Ceritinib比起克唑替尼使用限制要多一些。
Crizotinib不保护大脑?
Crizotinib特别的耐受?被用于一线alk+的进展的nsclc.
一个四期腺癌with all mutation 用Crizotinib 稳定了7个月。
曲美替尼,应对BRAF突变的靶向药。
NK细胞靶向。
免疫治疗与靶向药联用:
https://www.inspire.com/groups/a ... a-targeted-therapy/
Drug: Afatinib
Drug: Akt inhibitor AZD5363
Drug: Binimetinib BRAF-MEK-ERK
Drug: Crizotinib
Other: Cytology Specimen Collection Procedure
Drug: Dabrafenib BRAF
Drug: Dasatinib Abl,Src和 c-Kit
Drug: Defactinib FAK KRAS
Drug: FGFR Inhibitor AZD4547
Other: Laboratory Biomarker Analysis
Biological: Nivolumab
Drug: Osimertinib
Drug: Palbociclib CDK抑制剂 HER-2 ER
Biological: Pertuzumab
Drug: PI3K-beta Inhibitor GSK2636771
Drug: Sapanisertib MTOR PI3K
Drug: Sunitinib Malate PDGFR(PDGFRα和PDGFRβ),VEGFR(VEGFR1、VEGFR2、VEGFR3),FLT-3, CSF-1R,kit和ret
Drug: Taselisib PIK3CA HER2/neu
Drug: Trametinib MEK
Biological: Trastuzumab Emtansine HER-2+
Drug: Trk Inhibitor LOXO-101 TRK
Drug: Vismodegib Hedgehog信号通路
Drug: WEE1 Inhibitor AZD1775 铂类敏感 TP53
埃克替尼(凯美纳)是属于第一代针对EGFR靶点的国产靶向药物,与国外的易瑞沙和特罗凯属于相同药物。目前国际上已经批准的针对EGFR靶点二代的药物是阿法替尼、三代药物是Tagrisso(AZD9291);针对ALK的第一代药物是克唑替尼(赛可瑞),国际上已经有色瑞替尼和、阿雷替尼等;针对VEGF靶点的安维汀(贝伐珠单抗);另外还有一种很广谱的抗肿瘤药物,例如PD-1/PD-L1的免疫药物Opdivo,Keytruda和Tecentriq等。
9291+特罗凯,隔天184?
9291+280/克都可以考虑到CMET,而且光这个靶点,280/克的剂量由于副作用相对184低,剂量上可以更大
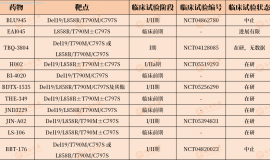
米哚妥林,c797s复合耐药突变。
西妥昔单抗+EAI045联用,西妥昔单抗单用对于仍有t790m突变的耐药患者并产生了c797s的部分有效(部分指?)
1、 体内仍然有不少T790m突变,9291 用60mg/d的剂量不足,这种情况就要考虑继续加量,60mg的量并不算大,如果副作用不大,可以考虑先加量到80mg;
2、体内有T790m突变的同时,仍然有EGFR突变存在,虽然9291对EGFR18、19、21也有作用,但是它的效力对比应该不会超过易、特、2992,或者60mg的9291 抑制不住EGFR突变,这种情况可以考虑联合易、特、(或者2992)曾经哪个有效果;
3、9291联合下游通路用药BKM120,BKM120不光是有PI3K突变,也是下游主要通路,肺腺癌病人中PI3K的突变率是2%,扩增率是6-19%;EGFR TKI联合BKM120可以克服HGF过表达导致的EGFR耐药问题,对于T790M或者cMet扩增导致的EGFR耐药病人,PI3K/Akt信号通路上调,EGFR TKI联合BKM120有一定效果。
4、体内T790m突变被清扫的差不多了,9291失去了作用的受体,完全耐药,换VEGFR靶点的阿西替尼、或者依托泊苷联合BKM120.
相关:http://www.yuaigongwu.com/thread-28922-1-1.html
5、如果有骨转或者CMET扩增的话,也可以考虑联合CMET药INC280、XL184、或则克唑替尼。
6、单药化疗;
2、 采用299804每天+9291隔天100mg
3、 盲试首先9291+易(或特),因较多为C797S突变。
299804 作用于HER-1/EGFR、HER-2、及HER-4。
Afatinib被推荐给进展性、转移性的EGF患者。对于EGFR mutation Del19有联用效果,L858R有小部分效果。
没突变考虑pd-1。
icotinib (凯美纳)对于脑转的治疗效果不错:
https://www.inspire.com/groups/a ... till-on/?ga=freshen
EGFR抑制剂有着更好的brain penetration (渗透)
erlotinib被认为有更好的效果对于脑部比起gefitinib
afatinib和osimertinib对于脑部效果比erlotinib好
Bevacizumab 与osimertinib 联合。
Dasatinib 对glioblastoma(exing胶质瘤)效果不错尤其是与afatinib和bevacizumab联用。
cetuximab, necitumumab (Portrazza) or bevacizumab跨越BBB并不容易,谨慎对待dasatinib for glioblastoma的实验结果。the BBB does not act the same way for glioblastoma and small brain metastases originating from NSCLC
艾乐替尼(alectinib)第二代ALK抑制剂,对脑转好像效果不错。
Pembro有过效果不错的例子。
osimertinib 交替卡铂+培美进行-对脑转很有效。
osimertinib 同时连续不断化疗。
Initial data from the ¬TATTON trial has found that osimertinib may be safely combined with a MET inhibitor (savolitinib) or a MEK inhibitor (selumetinib)。
Triple mutant cell lines 可能对哪代药都不敏感。
有两种药看起来对Triple mutant cell lines有效。(CUDC 1 0 1 和米哚妥林)
http://www.abstractsonline.com/pp8/#!/4292/presentation/5746
http://www.abstractsonline.com/p ... tions/osimertinib/1这个网址要通过insp进
osimertinib 和 crizotinib联用。
TMB与pd-1用药有关系。(mutational burden越高,免疫治疗有效的可能性越高)
对TKI治疗耐药,考虑下这个:
https://lungcancernewstoday.com/ ... 078ccd72b9-71328401
Tagrisso + Pemetrex
没有ALK ROS1突变不用克唑?
BRAF突变in addition EGFR Exon 20 selumetinib ,如果联用的话用dabrafenib 而不是azd2014。
单克隆抗体类:bevacizumab (Avastin) or ramucirimab (Cyramza)
ramucirimab 比bevacizumab副作用小
TKIs targeting VEGF-R are better than monoclonal antibodies.
TKI抑制VGFR:sorafenib, sunitinib, axitinib or apatinib.
2992对肺腺癌效果大。
gefitinib and afatinib 可以用于c797s double突变,Osimertinib 用于t790m double突变
关于brigatinib的信息:
http://www.nature.com/articles/ncomms14768?proof=true#results
brigatinib+ Osimertinib
brigatinib和西妥昔单抗联用比较好
除了对c797s之外,还可以考虑T790M loss 和 bypass pathway activation using existing treatment modalities, for example, turning back to first-generation EGFR–TKIs or combination therapy.
brigatinib和西妥昔单抗联用没有toxicity?
B+9291
Brigatinib和西妥昔单抗联用 IC50要小很多。
靶向药副作用比较也要考虑
Crizotinib打击三个靶点,副作用强有关于xiongshui 和食道的问题
如果考虑c met 的话 280与Osimertinib联用优于Crizotinib与Osimertinib联用
http://www.yuaigongwu.com/thread-29574-1-1.html 咨询
Lapatinib or Neratinib也许会是好的 TKI 在 C797S突变之后,因为占据atp site ?
爱必妥联用也许有重要性?
克唑替尼控制脑转移效果很有限,脑脊液浓度为血药浓度的0.26%。alectinib脑脊液浓度达到60%以上。
sclc的标准治疗是化疗。
T regulatory cells高了不好,和TILs有关系?
头盖放射延迟并发症:
https://www.uptodate.com/content ... cranial-irradiation
PD-L1 inhibitors such as Tecentriq (atezolizumab) or durvalumab的有效性,很大部分和pd-l1表达水平无关。
proton radiation therapy (质子放射治疗)容易产生高发生率的放射性坏死。
http://www.ajnr.org/content/early/2015/07/02/ajnr.A4333
Proton治疗最大程度的减小了放射超过肿瘤的范围,对于之前接受过传统放疗的部位很合适使用。
https://www.ncbi.nlm.nih.gov/pub ... with+scanned+charge d+particle+beams+Jensen
脑部治疗重复使用Gamma Knife可以?
Val-083 cells with p53, EGFR, or KRAS mutations were highly sensitive
新批准的胶质瘤药 对肺癌和其他癌症有一定效果
|
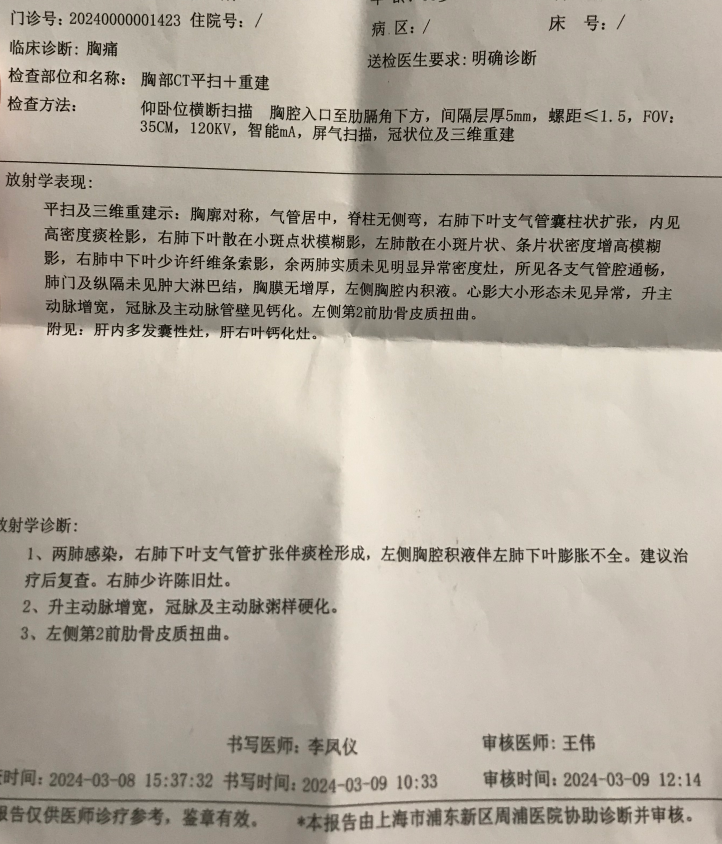 父亲生病一周年小记
2024年3月9日父亲感觉吸气的时候胸部有压迫感去卫生院做了个CT,CT还要经上级医院审
父亲生病一周年小记
2024年3月9日父亲感觉吸气的时候胸部有压迫感去卫生院做了个CT,CT还要经上级医院审
 母亲奥西耐药后应如何选择
2022年10月确诊肺腺癌,基因检测结果EGFR21,服用奥希替尼。2024年6月CT影像检查缓慢
母亲奥西耐药后应如何选择
2022年10月确诊肺腺癌,基因检测结果EGFR21,服用奥希替尼。2024年6月CT影像检查缓慢
 又一个肺癌四代靶向药倒下,奥希替尼
作者:闵
自第一款EGFR-TKI易瑞沙(即吉非替尼)于2005年在我国上市以来,EGFR-TKI药
又一个肺癌四代靶向药倒下,奥希替尼
作者:闵
自第一款EGFR-TKI易瑞沙(即吉非替尼)于2005年在我国上市以来,EGFR-TKI药
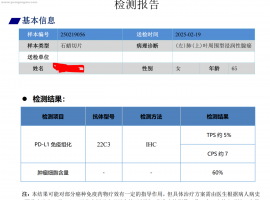 求助求助:妈妈的基因检测结果,EGFR
请版主帮忙@一下大神们,帮忙出一下注意。
帖子更新到2025年3月7日,首次手术样本,送
求助求助:妈妈的基因检测结果,EGFR
请版主帮忙@一下大神们,帮忙出一下注意。
帖子更新到2025年3月7日,首次手术样本,送
 奥希替尼联合卡马替尼进展求助
性别:女 年龄: 58 身高:155 体重:56kg 抽烟史:无
确诊时间:2021.2 确诊分
奥希替尼联合卡马替尼进展求助
性别:女 年龄: 58 身高:155 体重:56kg 抽烟史:无
确诊时间:2021.2 确诊分




 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡